"Uncover the truth behind the groundbreaking discovery of the causes of the world's biggest problems. 'The Root Causes' will change how you view the world!"
Minnesota Coronary Experiment Hidden from the Public and was Never Published for 43 Years.
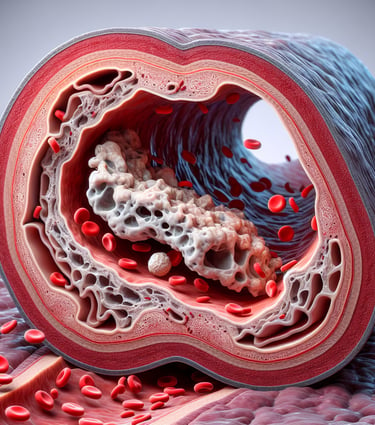
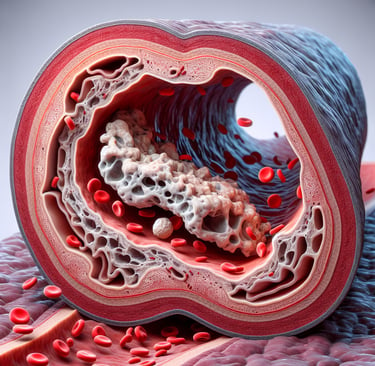
Our innovative studies on coronary health and laboratory advancements critically challenge the traditional diet-heart hypothesis, particularly regarding the role of saturated fats and vegetable oils rich in linoleic acid in coronary heart disease (CHD) prevention. The Minnesota Coronary Experiment (MCE), a landmark randomized controlled trial conducted between 1968-1973, revealed that while replacing saturated fat with linoleic acid reduced serum cholesterol levels, it did not improve survival rates. In fact, participants with larger cholesterol reductions faced higher mortality risks. This study, hidden for over 40 years, was only uncovered in 2016, revealing that previous conclusions about the diet-heart hypothesis were potentially overestimated due to incomplete data publication. A systematic review and meta-analysis of similar trials further supports that lowering cholesterol by replacing saturated fat with vegetable oils does not reduce mortality rates from coronary heart disease or all causes. These groundbreaking findings call for a reevaluation of long-held dietary guidelines.
DISEASES
Glenn Rosaroso Vale,BSMT, MS(IT), MBA
1/8/202513 min read


A Critical Re-evaluation of the Minnesota Coronary Experiment: Insights from Recovered Data (Hidden from the Public for 43 Yrs). Explore our innovative studies on coronary health and laboratory advancements.
This abstract summarizes a study that critically examines the traditional diet-heart hypothesis, which suggests that replacing saturated fat with vegetable oils rich in linoleic acid reduces coronary heart disease (CHD) and death by lowering serum cholesterol. The study focuses on the Minnesota Coronary Experiment (MCE), a randomized controlled trial (RCT) conducted between 1968 and 1973 that was never published to the public. Notably, this study was deliberately hidden for more than 40 years and was only released in 2016 when the leading estate investigator discovered the unpublished data in the basement of Ancel Keys, the researcher who initially introduced the manipulated data of the lipid hypothesis.
Key findings from the study include:
MCE Data: The intervention group in the MCE, which replaced saturated fats with vegetable oil rich in linoleic acid, experienced a significant reduction in serum cholesterol compared to the control group. However, this reduction did not translate into improved survival. In fact, for every 30 mg/dL reduction in serum cholesterol, there was a 22% increased risk of death. Participants who had greater reductions in cholesterol had a higher risk of mortality.
Systematic Review & Meta-analysis: The authors performed a systematic review and meta-analysis of randomized controlled trials (RCTs) that lowered cholesterol by replacing saturated fat with linoleic acid (from vegetable oils). They found no evidence of a mortality benefit from these interventions, either for coronary heart disease or all-cause mortality.
Conclusion: The study concludes that while replacing saturated fat with linoleic acid effectively lowers serum cholesterol, it does not reduce the risk of death from coronary heart disease or all causes. These findings challenge the traditional diet-heart hypothesis and suggest that previous positive results from trials, including MCE, were potentially overestimated due to incomplete publication of data.
Key Points:
The MCE data was hidden for over 40 years before being released in 2016.
Big Pharma's Statin Scam: The Dangerous Lies You’ve Been Told.
A SLIDE PRESENTATION that UNMASKS the lies behind heart disease treatment


The Statin Scam: Big Pharma’s Dangerous Lies About Heart Disease and Your Health"
The Truth About Statins – What Big Pharma Doesn’t Want You to Know!
For years, you've been told that statins are the ultimate solution for heart disease, but what if they’re actually doing more harm than good?
Here’s what Big Pharma isn’t telling you:
Statins don’t work for most people – Despite what you’ve been told, statins provide little to no benefit for those at low risk of heart disease.
Statins may actually promote heart attacks – Instead of preventing them, they could weaken your heart and damage your blood vessels.
Debilitating Side Effects:
Muscle pain
Memory loss
Fatigue
Liver damage
Dementia
Erectile dysfunction
Increased risk of diabetes – Statins can affect your blood sugar, increasing your risk of developing type 2 diabetes.
These harmful side effects are only the beginning. Statins don’t even address the real cause of heart disease, which is inflammation—not high cholesterol.
Rather than relying on these dangerous medications, there are safer, more effective ways to protect your heart and health.
This is urgent! The longer you stay on statins, the greater your risk of serious side effects and heart attack promotion. Don’t wait until it’s too late to make a change.
This presentation is for you if
§Taking Statin or any cholesterol-lowering drug §CVD §Diabetic taking statin §For young healthy individual who about to be prescribed with statin


2. Disclaimer
•Glenn Rosaroso Vale is not a doctor, but I have worked in the medical field for over 35 years in the laboratory. The information shared in this presentation is for informational purposes only and should not be taken as professional medical advice or recommendations. Please consult your healthcare provider before making any changes to your lifestyle or medical regimen based on this information."
•"The presenter and RootCausePrevention.com take no responsibility for any actions you may take based on the content presented in this webinar or the website. The information provided is meant to educate and inspire, not to diagnose, treat, or cure any medical conditions. Please always seek the advice of your physician or healthcare provider before acting on any information presented here."


Empower Yourself to Lead The Right Path To Reversal


3. Meet The presenter
Welcome You All in This Presentation
·My name is Glenn Rosaroso Vale, BSMT( MS(IT), MBA
·I have been in the medical field for more than 35 years
·Personal health challenges passionately motivate me to share with the world
·The presenter will debunk the cholesterol myth and stress how you have been lied to by Big Pharma for profits at the expense of your health.

4. WhaT IS STATIN? A CHOLESTEROL-LOWERING DRUG THAT CAUSES HORRIBLE MUSCLE PAIN, HEADACHE, FATIGUE DIABETES, AND PROMITES HEART ATTACK.
MODE OF ACTION OF STATIN AND ITS COLATERAL DAMAGE
Statin is a drug that blocks the enzyme HMG-Coenzyme Reductase in the upper cascade of the mevalonate pathway, thereby reducing cholesterol.
However, the same pathway also produces very important molecules, such as CoQ10, which is also reduced by statins. CoQ10 is the "spark plug" of the mitochondria and plays a crucial role in the production of energy in the form of ATP. This is why you may feel tired, fatigued, and experience muscle pain or muscle damage. Some people may even experience liver damage and other complications.
Additionally, the same mevalonate pathway produces a molecule necessary for insulin sensitivity called dolichol. A reduction in dolichol promotes diabetes.
Another molecule that is collateral damage is an isoprenoid called geranylgeranyl pyrophosphate, which is necessary for the conversion of Vitamin K1 to Vitamin K2. Reducing Vitamin K2 promotes heart attacks. Contrary to what Big Pharma promotes regarding preventing heart attacks, statins actually increase the risk of heart attacks due to the depletion of Vitamin K2.
And I’m not done yet. Since statins reduce LDL cholesterol, they also decrease testosterone production, causing your "toy" to go down below and become limp.
The side effects are dose-dependent. Lower dose might not feel any muscle pain at all but at cellular level , it slowly damaged your mitochondria

The Cholesterol Lie: Why We're Treating the Wrong Molecule
For decades, the medical community has focused on cholesterol as the primary culprit behind heart disease. Statin drugs, which lower cholesterol, are prescribed to millions of people worldwide with the belief that by reducing cholesterol levels, heart attacks and strokes can be prevented. However, recent scientific advancements have begun to expose a significant flaw in this narrative: we’ve been treating the wrong molecule.
Cholesterol itself is not the villain it's often made out to be. In fact, cholesterol is essential for numerous bodily functions, including the production of hormones, cell membranes, and vitamin D. Instead of cholesterol being the direct cause of heart disease, it’s more about how cholesterol behaves in the body and the underlying factors that affect its behavior. The real issue lies in the biochemical processes that produce and regulate cholesterol, as well as the molecules involved in these processes. Doctors are targeting the wrong culprit. It is not cholesterol that causes heart attacks; it's inflammation and oxidative stress.
One of the key molecules in question is Coenzyme Q10 (CoQ10), which is produced in the same metabolic pathway as cholesterol. CoQ10 plays a critical role in the production of energy within cells, particularly in the mitochondria. It acts like a "spark plug" for cellular energy, helping to produce ATP, the energy currency of the body. When statins lower cholesterol, they also inhibit the production of CoQ10. This reduction can lead to fatigue, muscle pain, and weakness—common side effects of statin use.
Furthermore, the mevalonate pathway, which is responsible for producing cholesterol, also produces other important molecules like dolichol (which is crucial for insulin sensitivity) and geranylgeranyl pyrophosphate, a molecule necessary for Vitamin K2 conversion. By disrupting this pathway, statins not only impact cholesterol levels but also create imbalances that can lead to diabetes, bone health issues, and an increased risk of heart attacks due to depleted Vitamin K2.
When statins lower LDL cholesterol, they might inadvertently lead to a reduction in testosterone production, contributing to symptoms such as low energy, loss of libido, and erectile dysfunction. While cholesterol levels are lowered, the overall biochemical balance of the body is disturbed, resulting in a cascade of unintended consequences.
Instead of focusing solely on cholesterol levels, we should be addressing the root causes of heart disease, such as inflammation, oxidative stress, and the overall biochemical health of the body. It's crucial to understand that cholesterol itself is not inherently harmful—it's the way the body processes and manages cholesterol that matters. By redirecting attention away from merely reducing cholesterol and instead focusing on improving the health of the entire metabolic system, we can find more effective and holistic solutions for heart disease prevention.
In conclusion, The Cholesterol Lie suggests that treating the wrong molecule—cholesterol—has misled both patients and doctors, leading to the widespread use of statin drugs with potential harmful side effects. It’s time to rethink our approach to heart health and focus on what truly matters in maintaining a healthy and balanced body.

Why cholesterol is a myth? Why is cholesterol a lie?
The Birth of a Lie
In the 1950s, an influential physiologist named Ancel Keys introduced his Lipid Hypothesis, asserting that eating a high-cholesterol diet could lead to heart attacks. To support his hypothesis, he conducted a study involving 22 countries. However, after gathering the data, he discovered that the results were scattered and did not produce a strong correlation. In response, he cherry-picked only 7 countries whose data aligned with his belief and discarded the 15 countries whose data did not match. By eliminating these 15 countries, the remaining 7 countries strongly supported his hypothesis, and his findings were popularized worldwide. The idea that cholesterol causes heart attacks spread like wildfire. Had the data been fully reported and not manipulated, the Lipid Hypothesis would never have existed.
When President Eisenhower suffered heart problems, his cardiologist was familiar with Ancel Keys' work, which led to the Lipid Hypothesis being adopted into U.S. food policy. It was endorsed by the USDA (United States Department of Agriculture) and the AHA (American Heart Association) in the food pyramid, which recommended a low-cholesterol diet.
In the 1980s, statins were developed to lower cholesterol, giving rise to a trillion-dollar statin industry. Even though these drugs targeted the wrong molecule, it didn’t matter because profits were made at the expense of public health.
In 2016, the leading investigator on Ancel Keys' death discovered a hidden document in a basement, related to a heart study called the Minnesota Coronary Experiment (MCE), which had been kept secret for 43 years. The findings of the MCE were never published. In his study, Keys initially aimed to demonstrate that reducing cholesterol could reduce heart attacks. However, the results of the MCE showed that reducing cholesterol did not decrease the mortality rate; in fact, it actually increased the mortality rate. People with LDL levels between 100-189 lived longer compared to people with normal or lower LDL cholesterol levels. The study revealed that for every 30 mg/dL reduction in LDL, there was a 22% increase in heart attacks, meaning that the lower your cholesterol, the shorter your life.
This study shows there is no benefit to lowering cholesterol—it’s a waste of time, money, and jeopardizes your health.
We hsve been lied for 43 years.
The Statistical Manipulation. How doctors being lied by big pharma?
Understanding the Statistical Methods: Relative Risk Reduction (RRR) vs Absolute Risk Reduction (ARR)
In clinical studies, two key statistical methods are often used to measure the effectiveness of a treatment: Relative Risk Reduction (RRR) and Absolute Risk Reduction (ARR). While both are used to quantify the benefits of a treatment, they present very different interpretations of the same data. Understanding the distinction between these two metrics is critical, especially when evaluating medications like statins, which are prescribed to millions of people based on their ability to reduce cholesterol and prevent heart disease.


Relative Risk Reduction (RRR) vs Absolute Risk Reduction (ARR)
Relative Risk Reduction (RRR):
Definition: Relative Risk Reduction is a measure used in clinical studies to express how much a treatment reduces the risk of an event (e.g., heart attack) relative to the baseline risk. It is calculated as the percentage reduction in the risk of the event in the treatment group compared to the control group.
Formula: RRR=Risk in Control Group−Risk in Treatment GroupRisk in Control Group×100\text{RRR} = \frac{\text{Risk in Control Group} - \text{Risk in Treatment Group}}{\text{Risk in Control Group}} \times 100RRR=Risk in Control GroupRisk in Control Group−Risk in Treatment Group×100
Interpretation: RRR expresses the percentage by which the risk is reduced in the treatment group compared to the control group. It is often used to show how effective a drug or intervention is in reducing the risk of a particular event, such as a heart attack.
Absolute Risk Reduction (ARR):
Definition: Absolute Risk Reduction is the actual difference in risk between the treatment group and the control group. It represents the real-world reduction in risk, showing how many fewer people experience an event in the treatment group compared to the control group.
Formula: ARR=Risk in Control Group−Risk in Treatment Group\text{ARR} = \text{Risk in Control Group} - \text{Risk in Treatment Group}ARR=Risk in Control Group−Risk in Treatment Group
Interpretation: ARR is the actual reduction in risk, indicating how many fewer people will experience the event in the treatment group compared to the control group. It is often seen as more meaningful when communicating the real benefits of a treatment to patients.
Example with Atorvastatin (Statin Drug)
In clinical trials for atorvastatin, the risk of heart attack (or cardiovascular events) is often measured using both RRR and ARR.
RRR of Atorvastatin: Statins like atorvastatin are shown to reduce the relative risk of heart attack by around 30-40%. So, if a study shows a RRR of 30%, this means that the risk of heart attack in those taking atorvastatin is 30% lower compared to those not on the drug.
ARR of Atorvastatin: However, the absolute reduction in risk might be much smaller. For instance, in a large population with a low baseline risk of heart attacks, the ARR might only be 1-2%. This means that out of 100 people taking atorvastatin, only 1-2 fewer people will actually have a heart attack compared to those who are not taking the drug.
Key Differences in Interpretation:
Relative Risk Reduction (RRR) focuses on the proportional difference in risk between the treatment group and the control group. It looks good because it highlights the effectiveness of a treatment in reducing risk on a percentage basis. For example, an RRR of 30-40% sounds fantastic because it suggests a significant reduction in heart attack risk. However, RRR is misleading—it doesn’t tell you how likely the event is to happen in the first place—it just shows the relative difference.
Absolute Risk Reduction (ARR) gives a clearer picture of the actual impact on an individual level. It tells you the real number of people who benefit from the treatment. While an RRR of 30-40% might sound like a big benefit, the ARR might only be 1-2%, meaning that only a few people out of a large group will actually experience the benefit. This is important because if the baseline risk of a heart attack is low, even a large RRR may still result in a small number of people avoiding an event.
Big Pharma's Manipulation of RRR
Big Pharma often uses Relative Risk Reduction in their marketing materials to make drugs, like statins, seem far more effective than they really are. They frequently print RRR in BIG BOLD LETTERS, highlighting the impressive 30-40% reduction in heart attack risk. This statistic looks fantastic and grabs attention. However, when you look closer at the Absolute Risk Reduction (ARR), the picture changes significantly. The ARR is often much smaller—only 1-2%. This means that despite the 30-40% relative reduction in risk, the actual benefit for an individual is minimal.
Summary:
RRR can exaggerate the perceived effectiveness of a treatment by focusing on proportional reductions.
ARR offers a more realistic understanding of the actual impact of a treatment, showing the tangible difference in outcomes for patients.
While Big Pharma loves to showcase the RRR of 30-40% in BIG BOLD LETTERS, the reality is that the ARR is only 1-2%, making the overall benefit much less significant than it first appears. This manipulation of statistics is crucial in understanding the true value—or lack thereof—of medications like statins. RRR is used by Big Pharma to convince doctors to prescribe these drugs by exaggerating the benefits, claiming a 30% to 40% risk reduction, which sounds appealing to their ears. However, in reality, they are downplaying the actual risks.

taking statin for nothing BUT get the side effectS
Fatigue and weakness
Headache
Muscle pain, myopathy, muscle death
Diabetes
Liver Damage
Dimentia
.Erectile Dysfunction
nikki martinez
My provider prescribed me a statin. When I took it, I experienced horrible muscle pain and headaches, so I decided to stop taking it. Thank God I was able to talk to Glenn Vake. I highly recommend buying his book Statin: The Silent Assassin. It will be worth it.


testimony
roegant de erio banlasan
My best friend in Manila experienced horrible headaches, fatigue, and muscle pain. She visited several doctors in Manila and had already spent millions of pesos on doctor visits, trying to find a solution. She transferred from one doctor to another, but no one was able to figure out what was wrong with her. At one point, I spoke to Glenn Vake about it, and he explained the devastating effects of statins. He suggested she stop taking the statin and try COQ10 and Vitamin K2. Within a week, her situation improved. She was very thankful to me. I recommend to buy his book Statin: The Silent Assassin.


testimony
12. Introducing My Book: statin: the silent aSSassin, EMPOWER YOURSELF WITH THE TOOLS AND KNOWLEDGE. GET THIS E-BOOK NOW
The book emphasizes the lies behind the lipid hypothesis and how you've been misled. It explains what happens to your body biochemically and how it causes damage.
This book will empower you to make the right decisions and avoid the scare tactics used by healthcare providers.
Act now—do not wait. The drug is dangerous and poisonous. It can kill you slowly.
Maybe I was like you before, ignoring the signs and symptoms of its poison.
13. Get the E-Book Today & Take Action
Don't fall victim to the devastating effects of the useless drug statin, which can lead to muscle pain, myopathy, rhabdomyolysis, increased risk of diabetes, dementia, heart attacks, fatigue, and a loss of energy. Take control of your health today and avoid these harmful side effects. Get your copy of the book now!
Thank
you FOR WATCHING THE presentation AND CLICK THE LINK TO PURCHASE THE BOOK
Glenn Rosaroso Vale, BSMT, MS(IT), MBA
903-268-6664
Health
Understanding illness to empower your well-being journey.
Wellness
Knowledge
info@rootcauseprevention.com
903-268-6664
© 2024. All rights reserved.
grfv@sbcgloal.net